Each tablet contains 800 mg sevelamer carbonate.
Excipients/Inactive Ingredients: Tablet core: Sodium chloride, Polyplasdone XL-10, Zinc stearate Powder USP, Purified Water.
Film-coating: Opadry White 03K285431, Alcohol 96%.
Pharmacotherapeutic group: All other therapeutic products, drugs for treatment of hyperkalemia and hyperphosphataemia. ATC code: V03AE02.
Pharmacology: Pharmacodynamics: Mechanism of action: SEVELAMER Symgens contains sevelamer, a non-absorbed phosphate binding cross-linked polymer, free of metal and calcium. Sevelamer contains multiple amines separated by one carbon from the polymer backbone which become protonated in the stomach. These protonated amines bind negatively charged ions such as dietary phosphate in the intestine.
Pharmacodynamic effect: By binding phosphate in the gastrointestinal tract and decreasing absorption, sevelamer lowers the phosphorus concentration in the serum. Regular monitoring of serum phosphorus levels is always necessary during phosphate binder administration.
Clinical efficacy and safety: In two randomised, cross over clinical trials, sevelamer carbonate in both tablet and powder formulations when administered three times per day has been shown to be therapeutically equivalent to sevelamer hydrochloride and therefore effective in controlling serum phosphorus in CKD patients on haemodialysis.
The first study demonstrated that sevelamer carbonate tablets dosed three times per day was equivalent to sevelamer hydrochloride tablets dosed three times per day in 79 haemodialysis patients treated over two randomised 8 week treatment periods (mean serum phosphorus time-weighted averages were 1.5 ± 0.3 mmol/l for both sevelamer carbonate and sevelamer hydrochloride). The second study demonstrated that sevelamer carbonate powder dosed three times per day was equivalent to sevelamer hydrochloride tablets dosed three times per day in 31 hyperphosphataemic (defined as serum phosphorus levels ≥ 1.78 mmol/l) haemodialysis patients over two randomised 4 week treatment periods (mean serum phosphorus time-weighted averages were 1.6 ± 0.5 mmol/l for sevelamer carbonate powder and 1.7 ± 0.4 mmol/l for sevelamer hydrochloride tablets).
In the clinical trials in haemodialysis patients, sevelamer alone did not have a consistent and clinically significant effect on iPTH. In a 12 week study involving peritoneal dialysis patients however, similar iPTH reductions were seen compared with patients receiving calcium acetate. In patients with secondary hyperparathyroidism sevelamer carbonate should be used within the context of a multiple therapeutic approach, which could include calcium as supplements, 1,25-dihydroxy Vitamin D3 or one of its analogues to lower the iPTH levels.
Sevelamer has been shown to bind bile acids in vitro and in vivo in experimental animal models. Bile acid binding by ion exchange resins is a well-established method of lowering blood cholesterol. In clinical trials of sevelamer, both the mean total-cholesterol and LDL-cholesterol declined by 15-39%. The decrease in cholesterol has been observed after 2 weeks of treatment and is maintained with long-term treatment. Triglycerides, HDL-cholesterol and albumin levels did not change following sevelamer treatment.
Because sevelamer binds bile acids, it may interfere with the absorption of fat soluble vitamins such as A, D, E and K.
Sevelamer does not contain calcium and decreases the incidence of hypercalcaemic episodes as compared to patients using calcium based phosphate binders alone. The effects of sevelamer on phosphorus and calcium were proven to be maintained throughout a study with one year follow-up. This information was obtained from studies in which sevelamer hydrochloride was used.
Paediatric population: The safety and effectiveness of sevelamer carbonate in hyperphosphatemic paediatric patients with CKD was evaluated in a multicenter study with a 2-week, randomised, placebo-controlled, fixed dose period (FDP) followed by a 6-month, single-arm, open-label, dose titration period (DTP). A total of 101 patients (6 to 18 years old with a BSA range of 0.8 m2 to 2.4 m2) were randomised in the study. Forty-nine (49) patients received sevelamer carbonate and 51 received placebo during the 2 week FDP. Thereafter all patients received sevelamer carbonate for the 26-week DTP. The study met its primary endpoint, meaning Sevelamer carbonate reduced serum phosphorus by an LS mean difference of 0.90 mg/dL compared to placebo, and secondary efficacy endpoints. In paediatric patients with hyperphosphatemia secondary to CKD, sevelamer carbonate significantly reduced serum phosphorus levels compared to placebo during a 2-week FDP. The treatment response was maintained in the paediatric patients who received sevelamer carbonate during the 6-month open-label DTP. 27% of paediatric patients reached their age appropriate serum phosphorus level at end of treatment. These figures were 23% and 15% in the subgroup of patients on hemodialysis and peritoneal dialysis, respectively. The treatment response during the 2-week FDP was not affected by BSA, in contrast however, no treatment response was observed in paediatric patients with qualifying phosphorus levels <7.0 mg/dL. Most of adverse events reported as related, or possibly related, to sevelamer carbonate were gastrointestinal in nature. No new risks or safety signals were identified with the use of sevelamer carbonate during the study.
Pharmacokinetics: Pharmacokinetic studies have not been carried out with sevelamer carbonate. Sevelamer hydrochloride, which contains the same active moiety as sevelamer carbonate, is not absorbed from the gastrointestinal tract, as confirmed by an absorption study in healthy volunteers.
In a clinical trial of one year, no evidence of accumulation of sevelamer was seen. However the potential absorption and accumulation of sevelamer during long-term chronic treatment (> one year) cannot be totally excluded.
Toxicology: Preclinical safety data: Non-clinical data with sevelamer reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity or genotoxicity.
Carcinogenicity studies with oral sevelamer hydrochloride were conducted in mice (doses of up to 9 g/kg/day) and rats (0.3, 1, or 3 g/kg/day). There was an increased incidence of urinary bladder transitional cell papilloma in male rats of the high dose group (human equivalent dose twice the maximum clinical trial dose of 14.4 g). There was no increased incidence of tumours observed in mice (human equivalent dose 3 times the maximum clinical trial dose).
In an in vitro mammalian cytogenetic test with metabolic activation, sevelamer hydrochloride caused a statistically significant increase in the number of structural chromosome aberrations. Sevelamer hydrochloride was not mutagenic in the Ames bacterial mutation assay.
In rats and dogs, sevelamer reduced absorption of fat soluble vitamins D, E and K (coagulation factors), and folic acid.
Deficits in skeletal ossification were observed in several locations in foetuses of female rats dosed with sevelamer at intermediate and high doses (human equivalent dose less than the maximum clinical trial dose of 14.4 g). The effects may be secondary to vitamin D depletion.
In pregnant rabbits given oral doses of sevelamer hydrochloride by gavage during organogenesis, an increase of early resorptions occurred in the high-dose group (human equivalent dose twice the maximum clinical trial dose).
Sevelamer hydrochloride did not impair the fertility of male or female rats in a dietary administration study in which the females were treated from 14 days prior to mating through gestation and the males were treated for 28 days prior to mating. The highest dose in this study was 4.5 g/kg/day (human equivalent dose 2 times the maximum clinical trial dose of 13 g/day, based on a comparison of relative BSA).
SEVELAMER Symgens is indicated for the control of hyperphosphataemia in adult patients receiving haemodialysis or peritoneal dialysis.
SEVELAMER Symgens is also indicated for the control of hyperphosphataemia in adult patients with chronic kidney disease (CKD) not on dialysis with serum phosphorus ≥ 1.78 mmol/l.
SEVELAMER Symgens should be used within the context of a multiple therapeutic approach, which could include calcium supplement, 1,25-dihydroxy Vitamin D3 or one of its analogues to control the development of renal bone disease.
Posology:
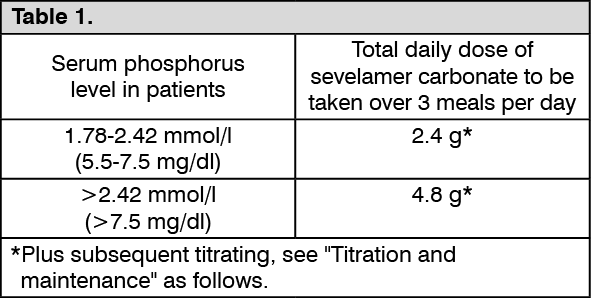
Starting dose: The recommended starting dose of sevelamer carbonate is 2.4 g or 4.8 g per day based on clinical needs and serum phosphorus level. SEVELAMER Symgens must be taken three times per day with meals. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
For patients previously on phosphate binders (sevelamer hydrochloride or calcium based), SEVELAMER Symgens should be given on a gram for gram basis with monitoring of serum phosphorus levels to ensure optimal daily doses.
Titration and maintenance: Serum phosphorus levels must be monitored and the dose of sevelamer carbonate titrated by 0.8 g three times per day (2.4 g/day) increments every 2-4 weeks until an acceptable serum phosphorus level is reached, with regular monitoring thereafter.
Patients taking sevelamer carbonate should adhere to their prescribed diets.
In clinical practice, treatment will be continuous based on the need to control serum phosphorus levels and the daily dose is expected to be an average of approximately 6 g per day.
Special populations:
Elderly population: No dosage adjustment is necessary in the elderly population.
Hepatic impairment: No studies have been performed in patients with hepatic impairment.
Paediatric population: The safety and efficacy of SEVELAMER Symgens in children below the age of 6 years or in children with a BSA below 0.75 m
2 have not been established. Not data are available.
The safety and efficacy of SEVELAMER Symgens in children over 6 years of age and a BSA >0.75 m
2 have been established. Current available data are described in Pharmacology: Pharmacodynamics under Actions.
For paediatric patients the oral suspension should be administered, as tablet formulations are not appropriate for this population.
Method of administration: Oral use.
Tablets should be swallowed intact and should not be crushed, chewed, or broken into pieces prior to administration. SEVELAMER Symgens should be taken with food and not on an empty stomach.
Sevelamer hydrochloride, which contains the same active moiety as sevelamer carbonate, has been given to normal healthy volunteers in doses of up to 14 grams per day for eight days with no adverse reactions. In CKD patients, the maximum average daily dose studied was 14.4 grams of sevelamer carbonate in a single daily dose.
The symptoms observed in case of overdose are similar to adverse reactions listed in Adverse Reactions, including mainly constipation and other known gastrointestinal disorders.
Appropriate symptomatic treatment should be provided.
Hypersensitivity to the active substance or to any of the excipients listed in Description; Hypophosphataemia; Bowel obstruction.
The safety and efficacy of sevelamer carbonate have not been established in adult patients with chronic kidney disease not on dialysis with serum phosphorus < 1.78 mmol/l. Therefore it is currently not recommended for use in these patients.
The safety and efficacy of sevelamer carbonate have not been established in patients with the following disorders: dysphagia; swallowing disorders; severe gastrointestinal motility disorders including untreated or severe gastroparesis, retention of gastric contents and abnormal or irregular bowel motion; active inflammatory bowel disease; major gastrointestinal tract surgery.
Treatment of these patients with SEVELAMER Symgens should only be initiated after careful benefit/risk assessment. If the therapy is initiated, patients suffering from these disorders should be monitored. SEVELAMER Symgens treatment should be reevaluated in patients who develop severe constipation or other severe gastrointestinal symptoms.
Intestinal obstruction and ileus/subileus: In very rare cases, intestinal obstruction and ileus/subileus have been observed in patients during treatment with sevelamer hydrochloride (capsules/tablets), which contains the same active moiety as sevelamer carbonate. Constipation may be a preceding symptom. Patients who are constipated should be monitored carefully while being treated with SEVELAMER Symgens. The treatment should be re-evaluated in patients who develop severe constipation or other severe gastrointestinal symptoms.
Fat-soluble vitamins and folate deficiency: Patients with CKD may develop low levels of fat-soluble vitamins A, D, E and K, depending on dietary intake and the severity of their disease. It cannot be excluded that sevelamer carbonate can bind fat-soluble vitamins contained in ingested food. In patients not taking supplemental vitamins but on sevelamer, serum vitamin A, D, E and K status should be assessed regularly. It is recommended that vitamin supplements be given if necessary. It is recommended that CKD patients not on dialysis are given vitamin D supplements (approximately 400 IU of native vitamin D daily) which can be part of a multivitamin preparation to be taken apart from their dose of sevelamer carbonate. In patients undergoing peritoneal dialysis additional monitoring of fat-soluble vitamins and folic acid is recommended, since vitamin A, D, E and K levels were not measured in a clinical study in these patients.
There is at present insufficient data to exclude the possibility of folate deficiency during long term sevelamer carbonate treatment. In patients not taking supplemental folic acid but on sevelamer, folate level should be assessed regularly.
Hypocalcaemia/hypercalcaemia: Patients with CKD may develop hypocalcaemia or hypercalcaemia. Sevelamer carbonate does not contain any calcium. Serum calcium levels should therefore be monitored at regular intervals and elemental calcium should be given as a supplement if required.
Metabolic acidosis: Patients with CKD are predisposed to developing metabolic acidosis. As part of good clinical practice, monitoring of serum bicarbonate levels is therefore recommended.
Peritonitis: Patients receiving dialysis are subject to certain risks for infection specific to dialysis modality. Peritonitisis a known complication in patients receiving peritoneal dialysis and in a clinical trial with sevelamer hydrochloride, a greater number of peritonitis cases were reported in the sevelamer group than in the control group. Patients on peritoneal dialysis should be closely monitored to ensure the correct use of appropriate aseptic technique with the prompt recognition and management of any signs and symptoms associated with peritonitis.
Swallowing and choking difficulties: Uncommon reports of difficulty swallowing the SEVELAMER Symgens tablet have been reported. Many ofthese cases involved patients with co-morbid conditions including swallowing disorders or oesophageal abnormalities. Proper swallowing ability should be carefully monitored in patients with co-morbid conditions. The use of sevelamer carbonate powder in patients with a history of difficulty swallowing should be considered.
Hypothyroidism: Closer monitoring of patients with hypothyroidism co-administered with sevelamer carbonate and levothyroxine is recommended (see Interactions).
Hyperparathyroidism: Sevelamer carbonate is not indicated for the control of hyperparathyroidism. In patients with secondary hyperparathyroidism sevelamer carbonate should be used within the context of a multiple therapeutic approach, which could include calcium as supplements, 1,25-dihydroxy Vitamin D3 or one of its analogues to lower the intact parathyroid hormone (iPTH) levels.
Inflammatory gastrointestinal disorders: Cases of serious inflammatory disorders of different parts of the gastrointestinal tract (including serious complications such as haemorrhage, perforation, ulceration, necrosis, colitis and colonic/caecal mass) associated with the presence of sevelamer crystals have been reported (see Adverse Reactions). Inflammatory disorders may resolve upon sevelamer discontinuation. Sevelamer carbonate treatment should be re-evaluated in patients who develop severe gastrointestinal symptoms.
Excipients: This medicine contains less than 1 mmol sodium (23 mg) per tablet, that is to say essentially 'sodium-free'.
Effects on ability to drive and use machines: Sevelamer has no or negligible influence on the ability to drive and use machines.
Pregnancy: There are no or limited amount of data from the use of sevelamer in pregnant women. Animal studies have shown some reproductive toxicity when sevelamer was administered to rats at high doses (see Pharmacology: Toxicology: Preclinical safety data under Actions). Sevelamer has also been shown to reduce the absorption of several vitamins including folic acid (see Precautions and Pharmacology: Toxicology: Preclinical safety data under Actions). The potential risk to humans is unknown. Sevelamer carbonate should only be given to pregnant women if clearly needed and after a careful risk/benefit analysis has been conducted for both the mother and the foetus.
Breast-feeding: It is unknown whether sevelamer/metabolites are excreted in human milk. The non-absorbed nature of sevelamer indicates that excretion of sevelamer in breast milk is unlikely. A decision on whether to continue/discontinue breast-feeding or to continue/discontinue therapy with sevelamer carbonate should be made taking into account the benefit of breast-feeding to the child and the benefit of sevelamer carbonate therapy to the woman.
Fertility: There are no data from the effect of sevelamer on fertility in humans. Studies in animals have shown that sevelamer did not impair fertility in male or female rats at exposures at a human equivalent dose 2 times the maximum clinical trial dose of 13 g/day, based on a comparison of relative BSA.
Summary of the safety profile: The most frequently occurring (≥ 5% of patients) adverse reactions were all in the gastrointestinal disorders system organ class. Most of these adverse reactions were mild to moderate in intensity.
Tabulated list of adverse reactions: The safety of sevelamer (as either carbonate and hydrochloride salts) has been investigated in numerous clinical trials involving a total of 969 haemodialysis patients with treatment duration of 4 to 50 weeks (724 patients treated with sevelamer hydrochloride and 245 with sevelamer carbonate), 97 peritoneal dialysis patients with treatment duration of 12 weeks (all treated with sevelamer hydrochloride) and 128 patients with CKD not on dialysis with treatment duration of 8 to 12 weeks (79 patients treatment with sevelamer hydrochloride and 49 with sevelamer carbonate).
Adverse reactions that occurred during clinical trials or that were spontaneously reported from post-marketing experience are listed by frequency in the table as follows. The reporting rate is classified as very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1,000), very rare (<1/10,000), not known (cannot be estimated from the available data). (See Table 2.)
Click on icon to see table/diagram/image
Paediatric population: In general, the safety profile for children and adolescents (6 to 18 years of age) is similar to the safety profile for adults.
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the national reporting system listed as follows.
United Kingdom: Yellow Card Scheme at: www.mhra.gov.uk/yellowcard or search for MHRA Yellow Card in the Google Play or Apple App Store.
Dialysis: Interaction studies have not been conducted in patients on dialysis.
Ciprofloxacin: In interaction studies in healthy volunteers, sevelamer hydrochloride, which contains the same active moiety as sevelamer carbonate, decreased the bioavailability of ciprofloxacin by approximately 50% when co-administered with sevelamer hydrochloride in a single dose study. Consequently, sevelamer carbonate should not be taken simultaneously with ciprofloxacin.
Ciclosporin, mycophenolate mofetil and tacrolimus in transplant patients: Reduced levels of ciclosporin, mycophenolate mofetil and tacrolimus have been reported in transplant patients when co-administered with sevelamer hydrochloride without any clinical consequences (e.g., graft rejection). The possibility of an interaction cannot be excluded and a close monitoring of blood concentrations of ciclosporin, mycophenolate mofetil and tacrolimus should be considered during the use of combination and after its withdrawal.
Levothyroxine: Very rare cases of hypothyroidism have been reported in patients co-administered with sevelamer hydrochloride, which contains the same active moiety as sevelamer carbonate, and levothyroxine. Closer monitoring of thyroid stimulating hormone (TSH) levels is therefore recommended in patients receiving sevelamer carbonate and levothyroxine.
Anti-arrhythmics and anti-seizure medicinal products: Patients taking anti-arrhythmic medicinal products for the control of arrhythmias and anti-seizure medicinal products for the control of seizure disorders were excluded from clinical trials. Therefore, possible reduction in absorption cannot be excluded. The anti-arrhythmic medical product should be taken at least one hour before or three hours after SEVELAMER Symgens, and blood monitoring can be considered.
Proton pump inhibitors: During post-marketing experience, very rare cases of increased phosphate levels have been reported in patients taking proton pump inhibitors co-administered with sevelamer carbonate. Caution should be exercised when prescribing PPI to patients concomitantly treated with SEVELAMER Symgens. The phosphate serum level should be monitored and the SEVELAMER Symgens dosage adjusted consequently.
Bioavailability: Sevelamer carbonate is not absorbed and may affect the bioavailability of other medicinal products. When administering any medicinal product where a reduction in the bioavailability could have a clinically significant effect on safety or efficacy, the medicinal product should be administered at least one hour before or three hours after sevelamer carbonate, or the physician should consider monitoring blood levels.
Digoxin, warfarin, enalapril or metoprolol: In interaction studies in healthy volunteers, sevelamer hydrochloride, which contains the same active moiety as sevelamer carbonate, had no effect on the bioavailability of digoxin, warfarin, enalapril or metoprolol.
Incompatibilities: Not applicable.
Special precautions for disposal and other handling: Any unused medicinal product or waste material should be disposed of in accordance with local requirements.
Keep the bottle tightly closed in order to protect from moisture.
This medicinal product does not require any special temperature storage conditions.
Shelf-life: 30 months.
V03AE02 - sevelamer ; Belongs to the class of drugs used in the treatment of hyperkalemia and hyperphosphatemia.
Sevelamer Symgens FC tab 800 mg
30's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image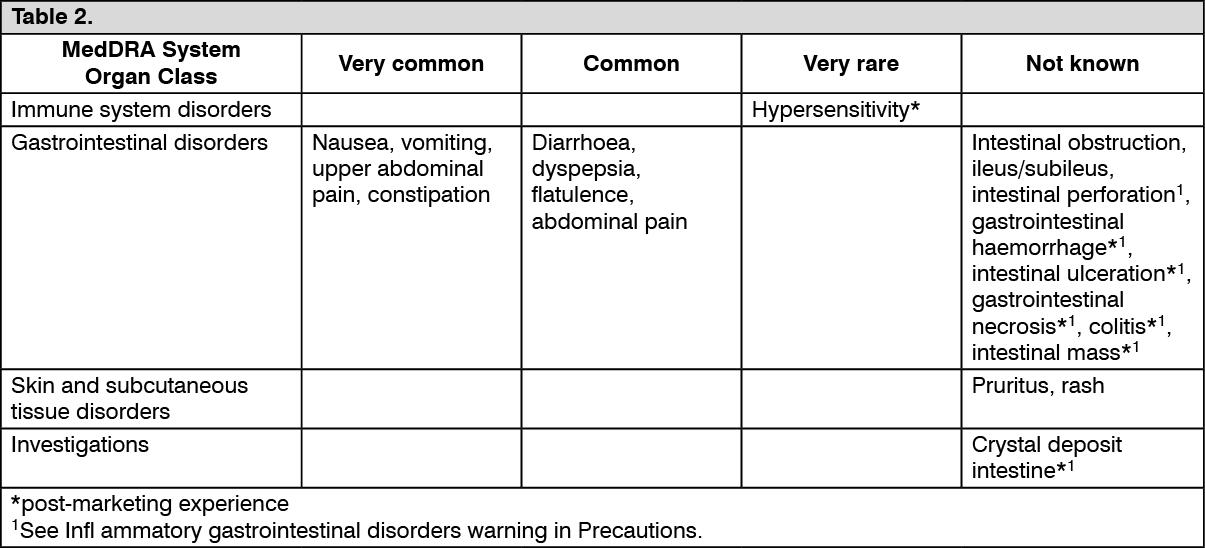 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out